
DOI: 10.20986/resed.2020.3767/2019
ORIGINAL
Quasi-experimental study on effectiveness of music therapy to reduce anxiety before an interventional technique at the pain unit
Estudio cuasi experimental sobre la efectividad de la musicoterapia para reducir la ansiedad ante una técnica intervencionista en la unidad del dolor
M. M. Monerris1, M. J. Medina Gómez2, A. Caparrós Giménez2, M. Aguas Compaired3 and M. J. Simón Solano1
1Servicio de Anestesiología, Reanimación y Terapéutica del Dolor. Hospital Universitario Sagrat Cor de Barcelona, España.2Departamento de Enfermería Quirúrgica. Hospital Universitario Sagrat Cor de Barcelona, España. 3Servicio de Farmacia Hospitalaria. Hospital Universitario Sagrat Cor de Barcelona, España
Received: 22-09-2019
Accepted: 13-01-2020
Correspondence: María del Mar Monerris
mmmonerris.germanstrias@gencat.cat
ABSTRACT
Objective: To assess the efficacy of music therapy in reducing anxiety in patients undergoing interventional technique (IT) in the Pain Unit (UD) of the University Hospital Sagrat Cor in Barcelona.
Material and method: Quasi-experimental study with a control group, prospective, pre- and post-intervention, transversal, non-randomized. Approved by the Research Ethics Committee IDC Salud Catalunya. Study population: patients scheduled to perform IT in the UD. Inclusion criteria: > 18 years old. IT indication. Exclusion criteria: psychiatric disorder, inability to answer study variables. Intervention group: IT has been performed by randomly playing the chosen music, free of noise pollution. Control group: IT has been performed without music therapy.
The modified analog visual scale has been used as a measuring instrument to assess the level of anxiety.
Results: 80 patients (71.6 % women, mean age 66.7 (SD 14) years, 49.4 % average studies, 64.2 % pensioners). 60.5 % do not perform treatment with anxiolytics. 59 % have low back pain, caudal epidural block is performed. 33.3 % underwent interventional technique for the first time.
In the control group the value of intra VAS is 5.83 (SD 3.2) and in the music therapy group 5.0 (SD 2.2), this difference is not statistically significant (F = 1.614, p = 0.208).
The same happens in the value of post-intervention EVA.
In the control group the value of post VAS is 3.7 (SD 3.3) and in the music therapy group 3.1 (SD 2.4), this difference is not statistically significant (F = 0.755, p = 0.387).
In the control group the value of the intra analog visual scale is 4.3 (SD 3.1) and in the music therapy group 3.0 (SD 2.0), this difference is statistically significant (F = 4, 83 p = 0.031).
In the control group the value of the post analog visual scale is 2.7 (SD 2.8) and in the music therapy group 1.3 (SD 1.5), this difference is also statistically significant (F = 7.427, p = 0.008).
81.5 % consider that they have received enough information about the interventionist technique and 18.5 % are satisfied.
95.1 % consider that the professionals have given him confidence and security and the remaining 4.9 % are considered satisfied.
Of those who have assessed (40 patients) if music has created a relaxed atmosphere, 80% are considered very satisfied and the remaining 20 % satisfied.
Conclusion: Although pain is not significantly improved in the interventionist group, anxiety does in both the intra and post-IT phases.
Patients feel very satisfied about the information received and consider the confidence and security provided by professionals very satisfactory. In addition, the music therapy group considers, in general, the relaxed atmosphere created by the music.
Music therapy is an excellent therapeutic tool, easy to use, accessible and economical, which can be used as an adjunct in IT in the UD.
Key words: Pain, anxiety, music therapy, interventional techniques.
RESUMEN
Objetivos: Valorar la eficacia de la musicoterapia en la disminución de la ansiedad en pacientes a los que se les realiza técnica intervencionista (TI) en la Unidad del Dolor (UD) del Hospital Universitario Sagrat Cor de Barcelona.
Material y método: Estudio cuasi experimental con grupo control, prospectivo, pre y postintervención, transversal, no aleatorizado. Aprobado por el Comité Ético de Investigación IDC Salud Catalunya. Población estudio: pacientes programados para realización de TI en la UD. Criterios inclusión: > 18 años de edad. Indicación de TI. Criterios exclusión: trastorno psiquiátrico, incapacidad contestar variables de estudio. Grupo intervención: se ha realizado la TI reproduciéndose aleatoriamente la música elegida, libre de contaminación acústica. Grupo control: se ha realizado la TI sin musicoterapia.
Se ha empleado la escala visual análoga modificada como instrumento de medida para valorar el nivel de ansiedad.
Resultados: 80 pacientes (71,6 % mujeres, media de edad 66,7 [SD 14] años, 49,4 % estudios medios, 64,2 % pensionistas). El 60,5 % no realiza tratamiento con ansiolíticos. El 59 % presenta lumborradiculalgia, se les realiza bloqueo epidural caudal. Al 33,3 % se les realiza técnica intervencionista por primera vez.
En el grupo control el valor de EVA intra es de 5,83 (SD 3,2) y en el grupo de musicoterapia de 5,0 (SD 2,2), esta diferencia no es estadísticamente significativa (F = 1,614, p = 0,208). En el valor de EVA postintervención sucede lo mismo.
En el grupo control el valor de EVA post es de 3,7 (SD 3,3) y en el grupo de musicoterapia de 3,1 (SD 2,4); esta diferencia no es estadísticamente significativa (F = 0,755, p = 0,387).
En el grupo control el valor de la escala visual analógica intra es de 4,3 (SD 3,1) y en el grupo de musicoterapia de 3,0 (SD 2,0), esta diferencia sí es estadísticamente significativa (F = 4,83, p = 0,031).
En el grupo control el valor de la escala visual analógica post es de 2,7 (SD 2,8) y en el grupo de musicoterapia de 1,3 (SD 1,5); esta diferencia también es estadísticamente significativa (F = 7,427, p = 0,008).
El 81,5 % considera que ha recibido suficiente información sobre la técnica intervencionista y el 18,5 % están satisfechos.
El 95,1 % considera que los profesionales le han aportado confianza y seguridad y el 4,9 % restante se consideran satisfechos.
De los que han valorado (40 pacientes) si la música ha creado un ambiente relajado el 80 % se consideran muy satisfechos y el 20 % restante satisfechos.
Conclusión: Aunque el dolor no se ve mejorado significativamente en el grupo intervencionista sí lo hace la ansiedad tanto en la fase intra como en la post TI.
Los pacientes se sienten muy satisfechos sobre la información recibida y consideran muy satisfactoria la confianza y seguridad que les aportan los profesionales. Además, el grupo de musicoterapia considera, en general, muy satisfactorio el ambiente relajado que les crea la música.
La musicoterapia es una excelente herramienta terapéutica, fácil de usar, accesible y económica, que puede utilizarse como coadyuvante en las TI en la UD.
Palabras clave: Dolor, ansiedad, musicoterapia, técnicas intervencionistas.
INTRODUCTION
Anxiety is an abnormal, overwhelming feeling of apprehension and fear, which leads physiological changes such as excess perspiration, hypertension and tachycardia. It is due to doubts about the reality and nature of the threat or because of the lack of self-confidence on the ability to deal with it (1,2).
There is currently a growing interest in alleviating the anxiety of patients (3) in any situation occurring in the hospital environment.
Musical intervention is a therapeutic resource that is increasingly being used as adjuvant therapy, to promote relaxation, emotional and spiritual comfort, distraction, feeling of well-being and pain relief (4).
Music has always been linked to the social life of humans, fulfilling different social functions (5). One of these functions is the application of music in medicine. In a hospital setting, music therapy has proven effective, mainly as a way to reduce anxiety (6).
When talking about music therapy, we mean how music can be used in a studied and controlled way to modulate the responses of the people who listen to it. These effects can be refreshing and sedative, anxiolytic, analgesic, etc. (7).
In an anxiety situation, breathing is usually blocked. Music can act as a guide to accompany and control breathing and help focus attention on the relaxation exercise (7), improving motivation and positive feelings of self-control against pain (8).
Several studies have shown the interaction between anxiety and pain. Anxiety is the most common form of impairment of subjective well-being in patients with chronic pain, highlighting the situational anxiety caused by situations such as invasive procedures (9).
Patients attending the pain unit frequently have stress and anxiety when undergoing an interventional technique.
A quiet and comfortable environment, without noise pollution, together with proper patient placement on the procedure table, are key points of care during the performance of an interventional technique. It requires knowledge of the health personnel, as well as being familiar with the programmed interventional technique. The interventional technique that will be performed, the drugs that will be administered, age, height, weight, patient history and safety measures (body position, the perfect functioning of the procedure table, the standards for patient protection and the anticipation of the needed equipment) should also take into account.
Rationale of the study
Bringuier (10), conducted in 2009 a comparative study of the use of the modified visual analog scale for anxiety with the State-Trait Anxiety Inventory for Children (STAIC) and the modified Yale Preoperative Anxiety Scale in the perioperative to measure anxiety in children aged 7 to 16 years, concluding that the modified visual analog scale for anxiety is a useful and valid tool (11).
One of the measuring tools that we will use to assess the level of anxiety in patients is the modified visual analog scale used in the Sepúlveda-Vildósola study (2014) on the use of music therapy to decrease anxiety in pediatric patients undergoing outpatient intravenous chemotherapy (2).
Chronic pain frequently triggers an anxiety picture, leading to a deterioration of subjective well-being in patients. When patients need some interventional technique and attend the pain unit, we notice a situational anxiety.
From the hospital setting it is essential to perform therapeutic measures to improve the comfort and safety of patients. Since there are currently no studies on the effectiveness of music therapy to reduce anxiety to an interventional technique at the Pain Unit, we consider that conducting this study is justified to demonstrate that music therapy is a useful and simple tool, which helps to reduce anxiety in people attending the Pain Unit to undergo an interventional technique.
Hypothesis
The music therapy used in those patients undergoing an interventional technique at the Pain Unit of the Sagrat Cor University Hospital in Barcelona decreases the level of anxiety.
Aims
The main objective is to assess the efficiency of music therapy in reducing the level of anxiety in those patients undergoing an interventional technique at the Pain Unit of the University Hospital Sagrat Cor in Barcelona.
As secondary objectives we tried: to assess the improvement in pain severity according to the visual analog scale, to quantify the variability in physiological parameters, to assess whether the collected variables modify the level of anxiety and to determine patient satisfaction after performing the interventional technique with music therapy.
MATERIAL AND METHODS
Study design
Quasi-experimental, controlled, prospective, non-randomized cross-sectional study.
Population and sample
The population under study are the patients scheduled two days a week, in the morning shift, for three months, to undergo an interventional technique at the Pain Unit of the Sagrat Cor University Hospital in Barcelona.
We found in the literature a reduction of severe anxiety from 70% to 20% in patients attending dental consultation after treatment with music therapy (11). A total of 33 patients would be needed for each group in this study for a unilateral test with a 95% confidence level, a statistical power of 80% and reduction of severe anxiety from 70% to 40%. Considering a lost to follow-up of these patients during the intervention can be a maximum of 15%, a total of 39 patients would be needed for each group.
Inclusion and exclusion criteria
The inclusion criteria are patients over 18 years of age and who have the indication of the interventional technique (blockages, radiofrequency). The exclusion criteria are patients with psychiatric disorder and/or unable to answer the study variables.
Description of the study variables
The variables included in the study are the following:
Description and development of the study
The recruitment of the patients has been as follows: the patients visited on afternoon on Tuesdays and Thursdays have been recruited for the intervention group (music therapy), the interventional technique was performed on Thursday morning. The patients visited on Wednesdays and Thursdays in the morning were recruited to the control group, the interventional technique was performed on Tuesday morning. In this way, patients were recruited in both the intervention group (music therapy) and in the control group during two days of visit per week and the interventional technique was performed by the clinician who visited them.
Patient recruitment was not randomized, but the study is prospective, controlled, and has followed the TREND (Transparent Reporting of Evaluations with Non-Randomized Designs) checklist published in 2004 (12).
On the day of the medical visit at the Pain Unit of the Sagrat Cor University Hospital in Barcelona, in which the interventional technique had been programmed, the patient received the “Patient Information Sheet” in addition to the “Informed Consent” and the “Informed consent of the interventional technique” to be performed. These consents are signed by the patient on day of the interventional technique. The information of both the interventional technique and the study is provided by the clinician who will subsequently perform the interventional technique.
The patient attends the Pain Unit of the University Hospital Sagrat Cor to undergo the interventional technique accompanied and with the above-mentioned signed consents.
The nursing staff collects the signed consents and subsequently the safety list is checked to perform the interventional technique: verification of the patient’s identity, allergies, correct withdrawal and/or replacement regimen in case of treatment with antiplatelet agents and/or anticoagulants for performing the technique and confirmation of the scheduled technique.
The patient goes to the changing room, where the appropriate clothes are provided to perform the interventional technique aseptically.
In the patients of the intervention group (music therapy), the room was kept with the doors closed and signs have also been made requesting silence to create a free of noise pollution area. The chosen music was randomly played using the Samsung Galaxy Tab A electronic device. A selection of 8 out of 184 melodies used in complementary and alternative medicine (13,14) was played randomly. They are described below: Mantra of Awalokaeshvara: The Meditative Sound of Buddhist Chants, Contemplation: Simply Karma Disc 1, Dreamers: Simply Karma Disc 1, One By One: A Day Without Rain (Enya), Flight Over Africa (John Barry), Beach At Night (John Barry), Over the Horizon: Brand Music and Mozart: Fantasia In D Minor.
Before performing the interventional technique, demographic data (age, sex, work activity, level of education) have been recorded, whether or not the patient is taking anxiolytics, the diagnosis and the interventional technique to be performed and if it is the first time that the patient is undergoing this technique.
Pain severity was evaluated according to the visual analog scale (VAS) and anxiety according to the modified visual analog scale. Simultaneously, vital signs (heart rate, non-invasive blood pressure and oxygen saturation by pulse oximetry) were recorded.
During the performance of the interventional technique (intra-intervention), the severity of pain is evaluated according to VAS and anxiety according to the modified visual analog scale, and vital signs (heart rate, non-invasive blood pressure and oxygen saturation by pulse oximetry) are recorded.
At the end of the interventional technique (post-procedure), the patient is transferred to the recovery room to monitor possible adverse effects and the severity of pain is reassessed according to VAS and anxiety according to the modified visual analog scale. Vital signs are also recorded (heart rate, non-invasive blood pressure and oxygen saturation by pulse oximetry).
Upon discharge of the patient from the Pain Unit of the Sagrat Cor University Hospital in Barcelona, a satisfaction questionnaire is also completed.
During all the time in which the patient has stayed at the Pain Unit, a pleasant environment has been maintained, without noise pollution, and the selection of melodies has been reproduced using the Samsung Galaxy Tab A electronic device.
In the patients of the control group, the interventional technique has been performed using the same methodology but no music therapy has been applied.
Data Collection
In a prospective and cross-sectional way, the variables described above have been collected by the nursing staff for later introduction into a database and subsequent analysis.
Data analysis
The recruitment period was three months (inclusion of the first case in June 2017, collection of the last case in February 2018).
A descriptive analysis has been conducted by calculating means and standard deviations of the quantitative variables and percentages of the qualitative variables.
To compare both groups of patients, the Chi-square test or Yates correction were used for the qualitative variables; whereas the Student’s t test for normal variables or the Man-Whitney U for of non-normally distributed variables or non-homogeneous variances were used in the case of quantitative variables.
A p value <0.05 is considered statistically significant.
The statistical application Statistics Package for the Social Sciences (SPSS) version 19.0 was used for the statistical data processing.
Ethical aspects
This study has been reviewed and approved by the Local Clinical Research Ethics Committee of the University Hospital Sagrat Cor in Barcelona (2017/13-UD-HUSC).
All study documents will be kept in the hospital file for a period of ten years after publication.
The project was performed following the guidelines indicated by the Good Clinical Research Practices and the Declaration of Helsinki and subsequent revisions (updated version at the 64th General Assembly, Fortaleza, Brazil, October 2013).
In compliance with Organic Law 15/1999, of December 13, on “Personal Data Protection”, the identity of patients should not be disclosed or revealed. Patients’ data collected througout the study are documented anonymously and in a dissociated way, linked to a code (center and patient number).
RESULTS
A total of 80 subjects have been recruited for the present study, 71.6% were women. The average age of the subjects was 66.7 (SD 14) years, 49.4% have completed high school and 64.2% are pensioners.
A total of 60.5% of subjects are not undergoing anxiolytic therapy.
59% of study participants have radicular low back pain and have undergone an epidural block.
The interventional technique was performed for the first time in 33.3% of the subjects.
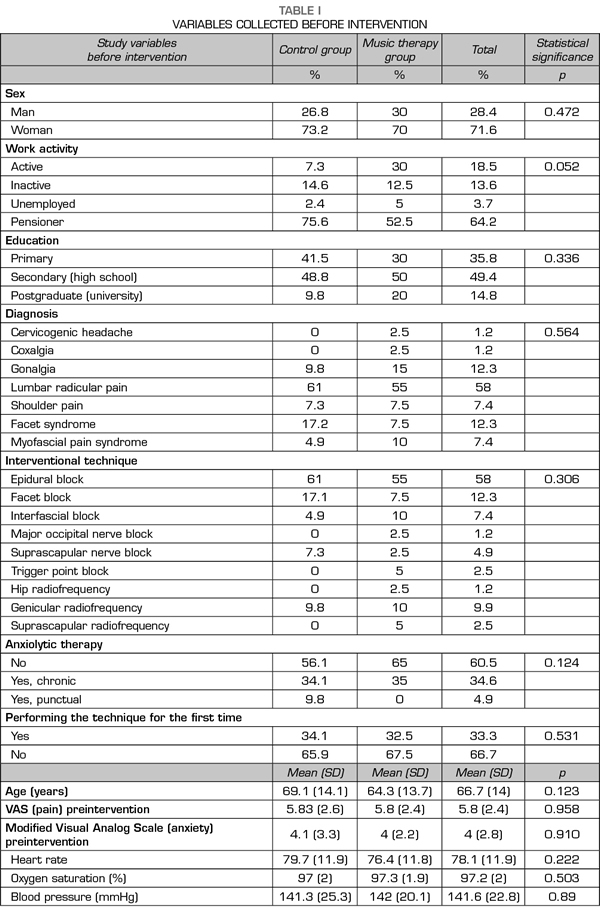
When comparing sex, age, work activity, level of education, diagnosis and interventional technique, prior treatment with anxiolytics, undergoing the technique for the first time, vital signs (heart rate, oxygen saturation and blood pressure), pain assessment according to the VAS and assessment of anxiety according to the modified visual analog scale before the interventional technique. No statistically significant difference was found between the patients in the control group and those who underwent music therapy intervention. That is, the groups are homogeneous and therefore comparable (Table I).
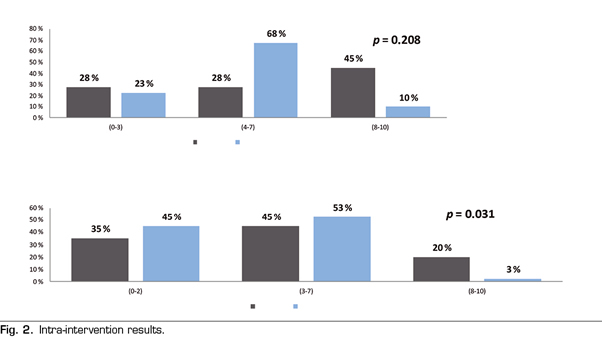
The intra-intervention VAS value in the control group was 5.83 (SD 3.2) and in the music therapy group it was lower, with a VAS value of 5.0 (SD 2.2). This difference is not statistically significant (F = 1.614, p = 0.208).
In the control group, the value of the intra-intervention modified visual analog scale (anxiety) was 4.3 (SD 3.1) and in the music therapy group it was lower, with a value of 3.0 (SD 2.0). This difference is statistically significant (F = 4.83, p = 0.031) (Figure 2).
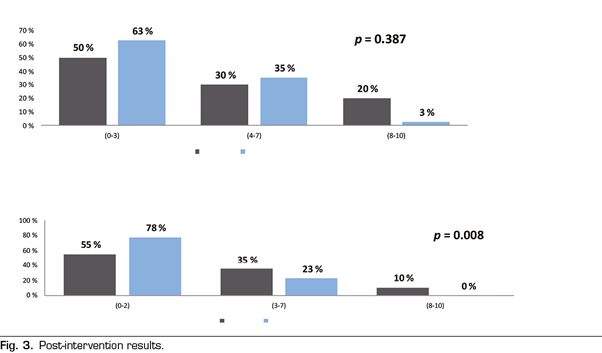
The same happens regarding the post-intervention VAS value. In the control group the post-intervention VAS value was 3.7 (SD 3.3) and in the music therapy group it was lower, with an VAS value of 3.1 (SD 2.4). This difference is not statistically significant (F = 0.755, p = 0.387).
In the control group the value of the post-intervention modified visual analog scale (anxiety) was 2.7 (SD 2.8) and in the music therapy group it was lower, with a value of 1.3 (SD 1.5). This difference is statistically significant (F = 7.427, p = 0.008) (Figure 3).
81.5% of the total subjects that participated in the study consider that they are very satisfied and 18.5% are satisfied that they have received enough information about the technique that has been performed.
95.1% of the total subjects who participated in the study consider that they are very satisfied and 4.9% are satisfied, since health professionals have given them confidence and security.
The subjects of the intervention group report that with the use of music therapy a relaxed environment has been created and 80% are considered very satisfied and the remaining 20% considered themselves satisfied.
DISCUSSION
Because patients attending the Pain Unit frequently present with anxiety, the purpose of this study was to demonstrate the importance of reducing the level of anxiety before performing an interventional technique at the Pain Unit.
Music therapy consists of an interaction between the healthcare professional, the patient, the music and the means used to offer it (2). Its purpose is to provide physiological, social, psychological and intellectual benefits to the patients to whom it is applied, reducing anxiety, which is associated with a state of negative stress, and increasing well-being (15).
A quiet and comfortable environment, without noise pollution, together with proper patient placement on the procedure table are key points of care during the performance of an interventional technique.
The International Association for the Study of Pain (IASP) defines pain as “an unpleasant experience associated with actual or potential tissue damage, it has sensory, emotional, cognitive and social components” (16). We have applied music therapy on the emotional component to reduce anxiety to an interventional technique (17).
To date, published studies (18-25) concerning anxiety, pain and music therapy have been performed in groups of patients undergoing endoscopy, cystoscopy and colposcopy, biopsy (breast, prostate), cures of burned patients, patients transplanted, women in labor and postpartum, surgeries (hip, knee, cardiac) and their postoperative, cancer patients and palliative care, patients undergoing extracorporeal shock wave lithotripsy, patients with multiple sclerosis, patients undergoing radiological procedures (nephrostomies, catheterizations) or other procedures (aesthetic, ophthalmological, dental, pleural). A decrease in anxiety levels and pain severity thanks to music therapy was found in all of them, either through a decrease in the requirements of anxiolytic and/or analgesic drugs.
We decided to use the modified visual analog scale of Sepúlveda-Vildósola (2) as a measure of anxiety level for several reasons: it is a scale that was used to assess the level of anxiety to a potentially stressful and painful technique; it is an easily understandable tool that can be completed quickly; and it adjusts to the times used in the performance of an interventional technique at the Pain Unit of the Sagrat Cor University Hospital in Barcelona.
The results obtained regarding the level of anxiety are similar to the studies of Bringuier (10) and Sepúlveda-Vildósola (2). These authors studied the level of anxiety in the pediatric population (7-16 years) who presented postoperative pain (10) or who was given intravenous chemotherapy (2). Both situations, obviously painful, generate a level of pre-, intra- and post-intervention anxiety.
We consider both studies extrapolated to the adult population, since in the age range (7-16 years), the subjects understand and express their anxiety levels, being almost comparable to the patients attending the Pain Unit of the Sagrat Cor University Hospital of Barcelona for the performance of an interventional technique.
In our study, through the use of music therapy, we found a clinically relevant improvement in pain severity measured by the VAS and a significant decrease in the anxiety measured by the modified visual analog scale at both intra-intervention and post-intervention (interventional technique) in the music therapy group.
Likewise, patients feel very satisfied about the information received and consider the confidence and security provided by health professionals as very satisfactory. In addition, the music therapy group considers that the relaxed atmosphere created by the music is in general very satisfactory.
Therefore, after assessing the results obtained in the present study, we consider that music therapy is an excellent therapeutic tool, easy to use, accessible and economical, with no adverse effects, which can be used as an adjunct in interventional techniques at the Pain Unit.
However, we cannot attribute the success of these results exclusively to music therapy. There are other external factors that may have influenced and that we must take into account (comfortable environment, area free of noise pollution, knowledge of health professionals and area where the interventional technique is performed).
For the future, according to the results obtained, we consider applying music therapy as a comprehensive part in the performance of interventional techniques at the Pain Unit of the Sagrat Cor University Hospital in Barcelona.
CONFLICTS OF INTEREST
Authors declared no conflicts of interest.
REFERENCES