DOI: 10.20986/resed.2018.3670/2018
ORIGINAL
Profiles of personality and resilience in chronic pain: utility of the cd-risc-10 to discriminate between resilient and vulnerable types
J. Soriano1 y V. Monsalve2
1Departamento de Personalidad, Evaluación y Tratamientos Psicológicos. Universidad de Valencia.
2Unidad Multidisciplinar para el Tratamiento del Dolor. Consorcio Hospital General Universitario de Valencia. España
Received: 05-03-2018
Accepted: 21-05-2018
Correspondence: José Soriano Pastor
jose.f.soriano@uv.es
INTRODUCTION
The classical definition of personality is related to the description, prediction and explanation of the intra-individual organization or structure of the subject (1). Personality is considered a system of interrelated traits susceptible to changes over time, although it is relatively stable (2). Currently the most widespread and accepted model establishes five big dimensions (Five-Factors Model [FFM]) composed of Neuroticism (N) (vulnerability, anxiety, depression), Extraversion (E) (gregariousness, excitement seeking, positive emotions), Openness ( O) (fantasy, values, tolerance to the unconventional), Agreeableness (A) (straightforwardness, trust, honesty) and Conscientiousness (C) (order, dutifulness, self-discipline) (3).
Two basic forms of research can be identified in the study and approach of personality relationships and their repercussions on the behavior of individuals: a) a more classical, dimensional approach or variable-centered approach, which seeks to describe the personality of the individual based on the scores obtained in various dimensions and the individual’s relationships and repercussions on behavior; and b) a person-centered approach, developed since the late 1990s, that seeks stable personality profiles based on the identification of types of individuals who share basic characteristics in these dimensions. The latter is based on the study of Block and Block (1980) on “ego-resiliency” and “ego-control” and suggested the existence of three personality profiles: resilient, overcontrolled and undercontrolled (4), which were initially identified by Robins et al. in children at the age of 13 and 14 years through the application of factor analysis with Q distribution (5). Following the theoretical framework of the FFM, the three-dimensional pattern was confirmed using principal cluster analysis, observing that the profile of the resilient group was characterized by being the most numerous and the best adjusted, while the overcontrolled group was more inhibited, with lower social self-esteem, more anxiety and more lonely (internalizing tendencies) and the undercontrolled tended towards antisocial behavior being more aggressive and with less social acceptance (externalizing tendencies) (5-7). These results have been corroborated in a review study in which 23,000 individuals were investigated using various assessment forms (2). These profiles involve interactions between traits that have been used as predictors of adjustment in several disorders (8,9). However, these profiles are not homogeneous through different studies and samples (10-12), even four profiles have been recently described (13). The replication problems may be due to the type of measurement of the FFM, type of analysis used, ethnicity, age or education level of the sample (14).
When we refer to the resilience construct, it should be noted that, although initially it referred to overcoming and adapting to situations of risk (15) or to their repercussions on family relationships (16,17), it is currently considered from a perspective of overcoming and of positive adaptation to stressors, stress and its main manifestations (18), considering that it is related to personality traits, results and processes (19). Therefore, it is established as a protective factor against adversity and negative emotions favoring the flexibility of adaptation and the overcoming of stressors (20). The characteristics of resilient individuals seem to contribute to a positive adjustment to problems by having a balanced vision of the subject’s life, perseverance, self-confidence, personal autonomy and meaning of life (21). It has also been considered as a trait when posed as the personality characteristics that moderate the negative effects of stress and promote adaptation (22,23).
From the variable-centered approach, resilience has been related to the five basic dimensions of personality, there are important associations between the dimensions O, C, N and E (24,25). Resilience has also been considered a good indicator of mental health (26). In cancer patients, resilience has been linked to a lower risk of suffering from psychiatric disorders (27).
In the case of chronic pain, currently defined as a disease, from the variable-centered approach, relationships have been found between the dimensions of personality, coping and pain (28,29), where N appears as the main dimension of vulnerability and the best predictor of maladaptive coping strategies and with E, O and C relating in the opposite direction in the adaptation of the patient with chronic pain to the illness and relating to a better quality of life (QoL) (30). In contrast, from the person-centered approach, maladaptive or vulnerable personality profiles have appeared, so that high scores in N, low in E, low O, moderate A and low C, have resulted in a worse quality of life in this type of patients (31,32). However, the existence of a personality profile clearly adaptive (resilient) to chronic pain is not clear. In addition, the undercontrolled profile that other studies have found in the non-clinical population (2,6) has not been identified in patients with chronic pain.
In chronic pain, resilience refers to both the ability to bounce back after the initial damage and to continue with normal functioning despite the repetition of problems (33). However, no references on whether resilience is related to personality profiles are available regarding chronic pain. Previous studies (31,32) address the issue of profiles where only two out of the three initially established profiles have appeared: a profile identified with the resilient and another identified with the overcontrolled although not totally coincident with the cited studies.
The objective of this study is to replicate the previously found profiles, to determine the differential capacity of resilience on these personality profiles evaluated using the Big Five model (FFM) and to determine its relation with the adaptation to the disease in patients with chronic pain.
MATERIAL AND METHOD
Sample
The sample consists of 494 patients diagnosed with chronic pain, Caucasian, who attend consecutively and for the first time at the Multidisciplinary Unit for the Treatment of Pain of the General University Hospital Consortium of Valencia.
All the patients had to be of legal age, meet the temporary pain criterion of more than 3 months of evolution, be able to complete the questionnaires and should not present any type of psychiatric/psychological disorder. All the participants gave their consent, after being informed, in order to be included in the study. The study has been approved by the Research Committee of the University General Hospital Consortium of Valencia.
Measurements
The measuring tools used were the following:
– Personality: The personality dimensions have been evaluated using the NEO-FFI questionnaire (34). Self-reported questionnaire of 60 items evaluated on a five-point scale from 0 (totally disagree) to 4 (totally agree). This questionnaire evaluates five personality dimensions: neuroticism (N), extraversion (E), openness to experience (O), agreeableness (A) and conscientiousness (C). The alpha values range from 0.70 (A) to 0.86 (N and E).
– Resilience: the 10-item version of the Connor-Davidson Resilience Scale (CD-RISC-10) questionnaire (35) was used. It is a 10-item self-reported questionnaire that is evaluated using a five-point scale from 0 (not at all) to 4 (always). It evaluates a single scale that refers to the personal traits that allow a person to face adverse situations (22). Its items refer to the personal perception of the abilities to adapt to change, management of unexpected situations, coping with the illness or management of negative feelings, among others (alpha 0.84).
– Coping: it has been evaluated with the Pain Coping Questionnaire (PCQ-R) (36,37). Self-reported questionnaire consisting of 24 items evaluated on a scale of five points from 1 (not at all) to 5 (totally). It is a pain coping questionnaire that evaluates 6 scales: distraction (not paying attention to pain), catharsis (search for emotional support), search for information (use of information to control pain), self-affirmation (encouragement without giving up), mental self-control (mental efforts to control pain) and religion (use of religion to obtain comfort). The alpha values range from 0.73 (distraction) to 0.95 (religion).
– Quality of life (QoL): evaluated with the SF-36 questionnaire (38). Although initially it was designed for the evaluation of the general health of the patient, it has been used as a measure of the quality of life in samples with patients with chronic pain (39). This is a self-reported measure that evaluates general health and is answered on a 5-point scale that varies according to the content of the items (there are inverted items). It consists of 36 items clustered into 8 scales: physical functioning (interference in physical activities such as self-care, walking, etc.), role-physical (problems with work or other daily activities), bodily pain (severity of pain and its effects on daily activities), general health (self-affirmation of current and future resistance to the disease), social functioning (interference in usual social activities), role-emotional (problems with work and others as a result of emotional problems) and mental health (anxiety, depression, behavioral and emotional control). The questionnaire has been validated in a Spanish sample (40).
– Intensity of pain: assessed using the visual analog scale VAS (41). It is a validated tool for measuring pain intensity (42). It consists of a line of 10 cm, where the subject has to indicate the intensity of pain on a scale of 0 to 10, representing zero “no pain” and 10 “the worst imaginable pain.”
Procedure
After the informed consent, the evaluation was performed in a session where the demographic data and information about the type of pain were collected; the above mentioned psychometric tests were performed. All the patients completed the questionnaires individually.
The data collection was performed after the type of pain was clinically diagnosed by the medical staff of the Multidisciplinary Unit for the Treatment of Pain of the Consortium of the General University Hospital of Valencia.
Following the person-centered approach, the cluster analysis technique has been used to form the groups. According to this technique, each individual is clustered from the five scores obtained in the NEO-FFI questionnaire (O, C, E, A, N) according to their similarity with the rest of the individuals. The Euclidean distance was used to obtain the profiles. Two phases were followed for the selection of the number of groups: first, a two-stage cluster analysis was conducted, which indicated the existence of two clusters. Subsequently, the subjects were classified using the K-means method, selecting two clusters. A second classification method was also tested, forcing the classification into three clusters (K-Means method), in order to replicate the results obtained in other studies (2,6). Once the groups were obtained, an ROC curve was used to establish the optimal cut-off point for the resilience variable that would allow the best separation between the groups of individuals based on their NEO-FFI scores. Finally, from this point on, the groups of individuals above and below that cut-off point were compared in their scores of coping and quality of life. The purpose of two and three clusters is to determine which solution may be the most useful and adjusted for patients with chronic pain.
For the reliable derivation of the prototypes (cluster), the procedure described by Blashfield and Aldenderfer (1988) (43) has been followed, which is the one used by other studies to replicate the solutions resulting from the cluster analyzes (6,44). The total sample was divided into two random parts in this procedure, being each of them analyzed separately. Subsequently, the solutions obtained from the clusters were compared by assigning the participants of each part to a new analysis using the Euclidean distances between their personality profiles and the centers of the other random group. The replication of these solutions was obtained by comparing the new clusters with the originals using Cohen’s κ coefficient (45). The recommendation of Asendorpf et al. (6) is a minimum agreement of κ = 0.60. In the present study, this condition was only obtained for the solution of two clusters, whereas the solution of three clusters was rejected (κ2 = 0.67 ***, κ3 = 0.05 **).
RESULTS
The average age of the sample is 52.56 (SD = 12.73); 42.3% (n = 209) are men, 91.5% (n = 452) live accompanied, 67.4 % (n = 333) have completed primary school (from 1 = can read and write, up to 4 = university education) and their distribution by type of pain indicates that 80% (n = 395) of them have pain associated with damage or alteration of the structures of the nervous system both peripherally and centrally (neuropathic pain) and 20% (n = 99) of them have pain associated with the stimulation of nociceptors by harmful stimuli (somatic pain).
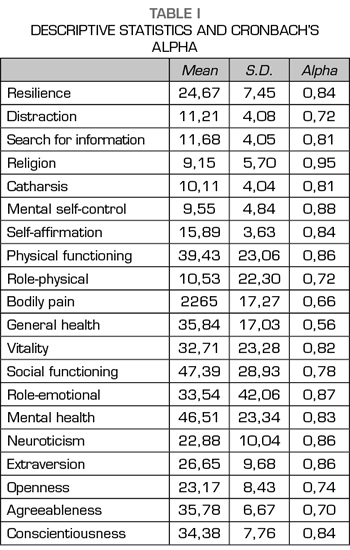
The levels of internal consistency obtained in each of the scales of the questionnaires are satisfactory except for the quality of life (QoL) scale for bodily pain and general health (Table I).
The descriptive statistics indicate that the average resilience score is similar to that obtained in other studies that used the same questionnaire with non-clinical samples, having all of them values around 27 (27,35,46). The scores obtained in coping strategies and quality of life are similar to those obtained with patients with chronic pain (31,32). Finally, the scores on the five personality dimensions indicate that the sample in general has a moderate N, low E and O, and high A and C (34).
Convergent validity
Resilience is significantly associated with personality dimensions, N (r = -0.59, p <0.000), E (r = 0.63, p <0.000), O (r = 0.38, p <0.000), A (r = 0.19,
p <0.000) and C (r = 0.56, p <0.000). The larger relationship between coping and resilience is established with self-affirmation (r = 0.62, p <0.000), moderately with distraction (r = 0.32, p <0.000) and low relationship is established with mental self-control
(r = 0 .22, p <0.000) and with information search
(r = 0.13, p <0.005). The most significant relationships with QoL are with mental health (r = 0.44, p <0.000), role-emotional (r = 0.36, p <0.000) and vitality
(r = 0.33, p <0.000) and low with general health
(r = 0.28, p <0.000) and social functioning (r = 0.27,
p <0.000).
Personality profiles: two and three clusters
Using the five dimensions of the NEO-FFI questionnaire and after performing a two-stage cluster analysis that indicated the presence of two groups, a cluster analysis (K-means) was conducted to obtain the maximum separation and description of the groups (Table II).
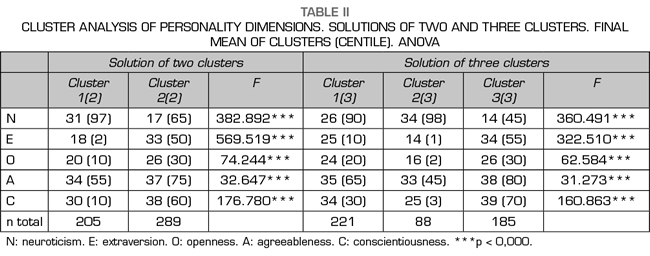
It can be observed that all the dimensions are suitable for a correct classification of the two clusters. Subsequently, a second K-means cluster analysis was performed selecting three clusters in order to replicate the previous studies that indicate the presence of three clusters according to the five personality dimensions (2,6).
Cluster 2 (2) and cluster 3 (3) would correspond to the designated as “resilient” in previous studies (2,6), which are characterized by average scores in N and E and high scores in C. Cluster 1 (2) and the Cluster 2 (3) correspond to the designated as “overcontrolled”, characterized by higher scores in N, low in E, O and C and moderate in A. The designated as cluster 1 (3) in the solution of three clusters has similarities with the designated as overcontrolled, with the difference of having a moderate score in A (Table II).
Due to the large coincidence in the solution of three clusters between clusters 1 (3) and 2 (3), as well as to the low score obtained in Cohen’s Kappa coefficient after randomization of the subjects, it was decided to continue with the solution of two clusters (Figure 1).
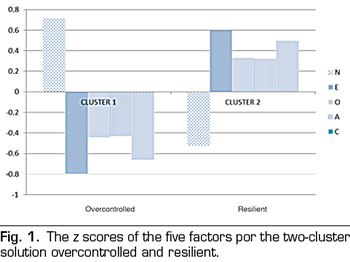
Focusing on the solution of two clusters, the scores of each cluster for the resilient variable have been compared between the two profiles, where significant differences appear, scoring significantly lower in the first cluster (Cl1 M = 29, SD = 6.6, Cl2 M = 37.9,
SD = 5.7, F = 6.22, p = 0.000, d = 0.25).
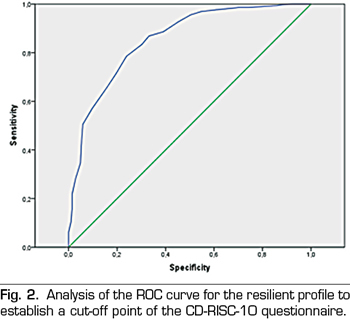
Adjustment of resilience delimitation on the resilient personality profile
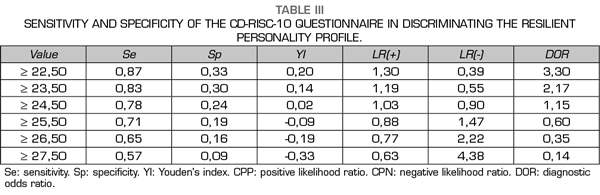
From the two established personality profiles, a ROC curve based on the total score for resilience (CD-RISC-10) on the profile of resilient personality was performed. AUC was 0.85 (p <0.000, 95% CI = 0.82-0.88), indicating that the CD-RISC-10 has a good fit to detect the profile obtained with the NEO-FFI. Figure 2 shows the graphical representation of the curve between sensitivity and 1-specificity. Table III shows the personality adjustments, being the optimal cut-off point ≥ 25.
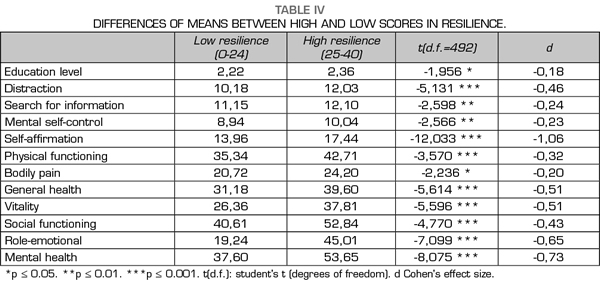
To determine the discrimination capacity of the CD-RISC-10 questionnaire from the established cut-off point (high resilience ≥ 25), the sample has been divided again into two clusters, calculating the differences between coping strategies and quality of life. Therefore, the sample is divided into two clusters according to whether or not they exceed this cut-off point.
The results shown in Table IV only include the significant differences regarding VAS, age, level of education, coping and quality of life. There are no significant differences in age and despite there are differences in level of studies, the effect size (Cohen’s d) indicates its low relevance. An important aspect to note is that there are no significant differences in initial VAS of pain. In coping, self-affirmation is the measure obtaining the largest difference, followed by the distraction strategy and with a smaller effect the search for information and high mental control. In QoL the biggest difference appears in the scale of mental health, along with role-emotional, vitality and general health. To a lesser degree, there is social function, physical function and bodily pain.
Finally, a multiple regression analysis (stepwise, F to enter ≤ 0.05 and F to remove ≥ 0.10) was performed to determine to what extent the personality dimensions evaluated with the NEO-FFI were able to explain the scores obtained in resilience. The results indicate a good multivariate prediction (R2 = 0.56, F = 153.588, p = 0.000). Only four of the dimensions were included in the equation, leaving out the dimension A:
N (B = - 0.225, p = 0.000), E (B = 0.225, p = 0.000),
C (B = 0.248, p = 0.000), and O (B = 0.109,
p = 0.000). The Durbin-Watson value (autocorrelation of residues) was within the accepted range (1.847).
DISCUSSION
One of the problems of evaluation in health psychology is the relationship between the limited time available and the number of tools used to evaluate the patient’s adaptation to illness. At the same time, it is necessary to determine from what point a dimension or variable can become a potential risk or resistance for the individual. In the case of chronic pain, there are often no techniques available to eliminate pain, so the patient must learn to adapt to it. All this implies the need to use variables that can be anticipate if the subject has a larger or lesser probability of being able to adapt to his/her condition as a chronically ill person.
A research line, developed since the 1990s, involved taking into account stable variables of temperament that could foresee some of these traits (O, C, E, A, N). Following this line, the results of the present study indicate that the N dimension is the best representing the vulnerability of individuals; E, O and C act as protective factors and dimension A is the poorest for these purposes, traits that are widely known in the reference literature (47,48).
At the same time that interest in temperament was developed, a variable that has been transformed over time has appeared: resilience. Although controversial and criticized, it has generated some interest in studies on chronic pain (33). This variable has been related to the temperamental dimensions and coping in non-clinical populations (24,25,35,49), showing a negative relationship with N and a positive relationship with E, C and O, being the weakest relationship with A , aspects that have been replicated in the present study.
The personality profiles derived from the FFM model are less studied in chronic pain. Despite the initial studies found three profiles (4-6,50), this study could not verify them, similarly occurred with other studies that have not achieved it (51,52), considering that the types associated with problematic results (overcontrolled and undercontrolled) may be underrepresented in certain types of samples (50). Consistently with previous studies (31,32), only two groups, clusters or reliable profiles could be obtained: a profile that we can denominate resilient and another profile that was denominated vulnerable (overcontrolled). The nomenclature used is based on the comparison of the results with previous studies, so that the resilient profile obtained with two and three clusters tends to be consistent with other studies in which there is coincidence with low score in N, high in E and C and moderate in O and A (12,53). However, the overcontrolled profile only coincides with the dimensions of high N and low E, tending the others toward low scores instead of intermediate ones. Finally, in the three cluster model, the least coincident profile is the undercontrolled one, especially in C that appears intermediate and E, O and A change in relation to the scores obtained by other studies, N being the one that best matches. In spite of the inconsistencies obtained in multiple studies with the overcontrolled type (see Alessandri et al., 2013 [54], for a review), the general conclusion is that this profile presents high behavioral inhibition and acts with caution when facing new stressful situations obtaining scores “socially undesirable” and cluster individuals with higher levels of anxiety and depression (50,55). An explanation of the results obtained may be that the chronification of pain, understood as a stressor, is easier to identify in two types mainly (though perhaps not only in two). The undercontrolled cluster, which is more characterized by more aggressive behavior, less empathic and with little conscientiousness, is not a clear profile that appears in the clinical consultation with ease; and it may involve a selection bias due to its lack of identification and adherence to the problem. However, the avoidant individual, with anxiety and depression (vulnerable or overcontrolled), similarly to the resilient, are easily identifiable. This can be considered as differential characteristics in the sense of sharing a stressor such as the chronification of pain, present in most diseases. In fact, there is currently an important discussion regarding the inclusion of “distress” in the definition of pain (56). Another parallel problem is the origin; we know that it is derived from genetics and the environment (57).
Once the two profiles have been identified (resilient and vulnerable or overcontrolled) and considering the previously results obtained, the question arises of trying to establish the discrimination of the profiles based on an external score of resilience. First, it should be noted that the mean resilience score is similar to that shown in other studies with other populations (27,35,46), all of them around 27. For the separation of the groups, the cut-off point was set at 25 through the ROC curve, obtaining a good discrimination (AUC = 0.85). This result indicates that resilience, evaluated using CD-RISC-10, can provide a prediction about the profile (resilient or vulnerable) of the patient, which points out to the relationship between the personality traits studied using profiles and the resilience in patients with chronic pain. This does not mean that resilience is a fixed trait or acts exclusively as a fixed trait, but that the score obtained with this questionnaire allows a good discrimination. Furthermore, although resilience is considered a trait, it could be malleable (58). This result is not strange when looking at the items that compose the questionnaire, which refer to self-efficacy, assessment of challenge or coping focused on the problem, among others, aspects that individually have already been described in previous studies and obtain similar relationships to those obtained in the present study (24,25).
Its utility is established when the sample is divided into two clusters based on the cut-off point where significant and important differences appear between both clusters, especially in several QoL dimensions and, very remarkably, in the coping strategy of self-affirmation, which has shown to be the most important in QoL at pain (36,37).
Furthermore, the fact that resilience is explained at a multivariate level by just over 50% from four of the dimensions of the NEO-FFI indicates the clear relationship of resilience with them. It is worth noting the contribution of dimension C, which indicates that the implication, order or need for achievement are the best predictors of resilience score, being followed by N and E with similar contributions and less by O. As expected, dimension A is excluded from the equation. As indicated above, these results are consistent with studies published previously.
As points to consider, we should indicate that the possibility of obtaining two groups instead of three may also be related to age, since the original studies used to use ages that did not exceed 30 years, whereas in the present study the average age is over 50 years (5,6,53). Another possibility is the type of questionnaire used to evaluate the personality dimensions for obtaining the profiles (14,59), the methodology for obtaining the groups (Q-type factor, cluster analysis or latent profile) or the method used for data collection (44).
It should be noted that this study does not propose the existence of a personality profile predisposing to chronic pain, as stated in other studies (60), but we only suggest the utility of 10-item measure when classifying the patients and to anticipate, based on the high relationship with their personality profiles, the consequences that chronic pain can have on both their quality of life and the use of coping strategies applied to their illness.
CONFLICTS OF INTEREST
Authors declare no conflicts of interest.
BIBLIOGRAPHY